Understanding and Managing Varicella-Associated Abscesses: A Comprehensive Guide
Chickenpox, caused by the varicella-zoster virus (VZV), is generally a self-limiting illness. However, scratching the characteristic itchy blisters can introduce bacteria, leading to secondary skin infections, including abscesses. This guide details the diagnosis, treatment, and prevention of these potentially serious complications.
Diagnosing the Problem: Recognizing Varicella-Associated Abscesses
Clinical Presentation: Spotting the Signs
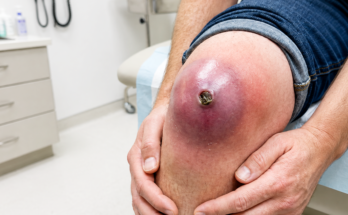
Identifying a varicella-associated abscess begins with recognizing the clinical picture. Patients typically present with a history of recent chickenpox, characterized by fever and an itchy, vesicular rash. The abscess itself will appear as a localized area of redness, tenderness, and swelling, often containing pus (fluctuance). The area may feel warm to the touch. These signs are often sufficient for a clinical diagnosis.

Confirming the Diagnosis: Investigations When Necessary
While clinical presentation often suffices, additional investigations may be necessary for confirmation or to guide treatment. An ultrasound can differentiate an abscess from cellulitis. A culture of the pus, obtained through incision and drainage (I&D), identifies the specific bacteria responsible, allowing for targeted antibiotic therapy. In cases of suspected systemic involvement, a complete blood count (CBC), C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) may be helpful to assess the extent of inflammation.

Treating Varicella-Associated Abscesses: A Multi-pronged Approach
The management of varicella-associated abscesses requires a comprehensive strategy addressing both the viral and bacterial components of the infection.
Targeting the Bacterial Infection: Antibiotic Therapy
Antibiotic selection depends on the suspected pathogen and the severity of the infection. Empiric therapy, initiated before culture results are available, usually targets Staphylococcus aureus (including methicillin-resistant S. aureus – MRSA) and Streptococcus pyogenes. Outpatient treatment might involve clindamycin or a combination of trimethoprim-sulfamethoxazole (TMP-SMX) and amoxicillin. For inpatient treatment of moderate to severe cases, or where MRSA is suspected, intravenous vancomycin or linezolid are preferred. Once culture results are available, the antibiotic regimen can be narrowed to match the specific pathogen. For Streptococcus pyogenes, penicillin G combined with clindamycin is often effective. Clindamycin’s ability to inhibit toxin production is beneficial. The typical duration of antibiotic therapy is 7-14 days, depending on the severity and response to treatment.
Draining the Abscess: The Role of Incision and Drainage

Incision and drainage (I&D) is the cornerstone of abscess management. This procedure involves making a small incision to release the pus, followed by irrigation and, if necessary, packing the wound. I&D is particularly important for abscesses larger than 1 cm, those that are fluctuant (easily palpable fluid), or those that don’t respond adequately to antibiotics alone. The pus should also be sent for culture to confirm the bacterial species. Post-I&D care includes warm compresses, regular dressing changes, and careful monitoring for recurrence or the development of cellulitis.
Addressing the Viral Infection: Antiviral Therapy

If the varicella infection itself is active and severe, or if the patient is immunocompromised, antiviral therapy is indicated. Acyclovir, either orally or intravenously (for severe cases), and valacyclovir (with better oral bioavailability) are the primary agents used. The dosage and duration of treatment are determined by the severity of the varicella infection.
Supportive Care: Enhancing Recovery

Effective management includes supportive measures. Pain management is essential using appropriate analgesics. Maintaining adequate hydration is crucial. Good hygiene practices help prevent the spread of infection. Importantly, NSAIDs (like ibuprofen) should be avoided, as they may increase the risk of severe skin complications.
When to Seek Immediate Medical Attention
Certain situations warrant immediate medical evaluation and potential hospitalization. These include:

- Deep tissue involvement (e.g., necrotizing fasciitis)
- Signs of systemic infection (fever, tachycardia, hypotension)
- Immunocompromised individuals
- Failure to respond to outpatient therapy
Preventing Varicella and its Complications: The Power of Vaccination
Vaccination against varicella is highly effective in preventing both the primary infection and secondary bacterial complications. The recommended vaccination schedule typically involves two doses: the first between 12 and 15 months of age, and the second between 4 and 6 years of age.
This comprehensive guide provides a detailed overview of varicella-associated abscesses, emphasizing the importance of timely diagnosis and appropriate management to ensure optimal patient outcomes. Always consult with a healthcare professional for diagnosis and treatment.